By Rose O. Sherman, EdD, RN, NEA-BC, FAAN
CNOs quietly tell me that they are under enormous pressure from their C-Suite colleagues. Nurse staffing improved in almost every health system in the country in 2025, yet these staffing gains are not translating into improved care and performance metrics. Despite our sophisticated technology and increased staffing, our “Never Event” protocols, and our relentless focus on quality, patient safety feels more fragile than ever. I hear the same concern: “We are doing more than ever to keep patients safe, yet it feels like we’re losing ground.”
There is an explanation for what you are seeing. Yes – we may have our vacancies filled and rely less on contract staff, but even AHA in the 2026 hospital scan report noted that our workforce stability is very fragile. Acute care environments are admitting older and more acutely ill patients who present higher risks. The volumes and turnover of patients are like nothing we have ever experienced in healthcare. At the same time, the care complexity-staff experience gap continues to widen as more novices join the acute care workforce each year.
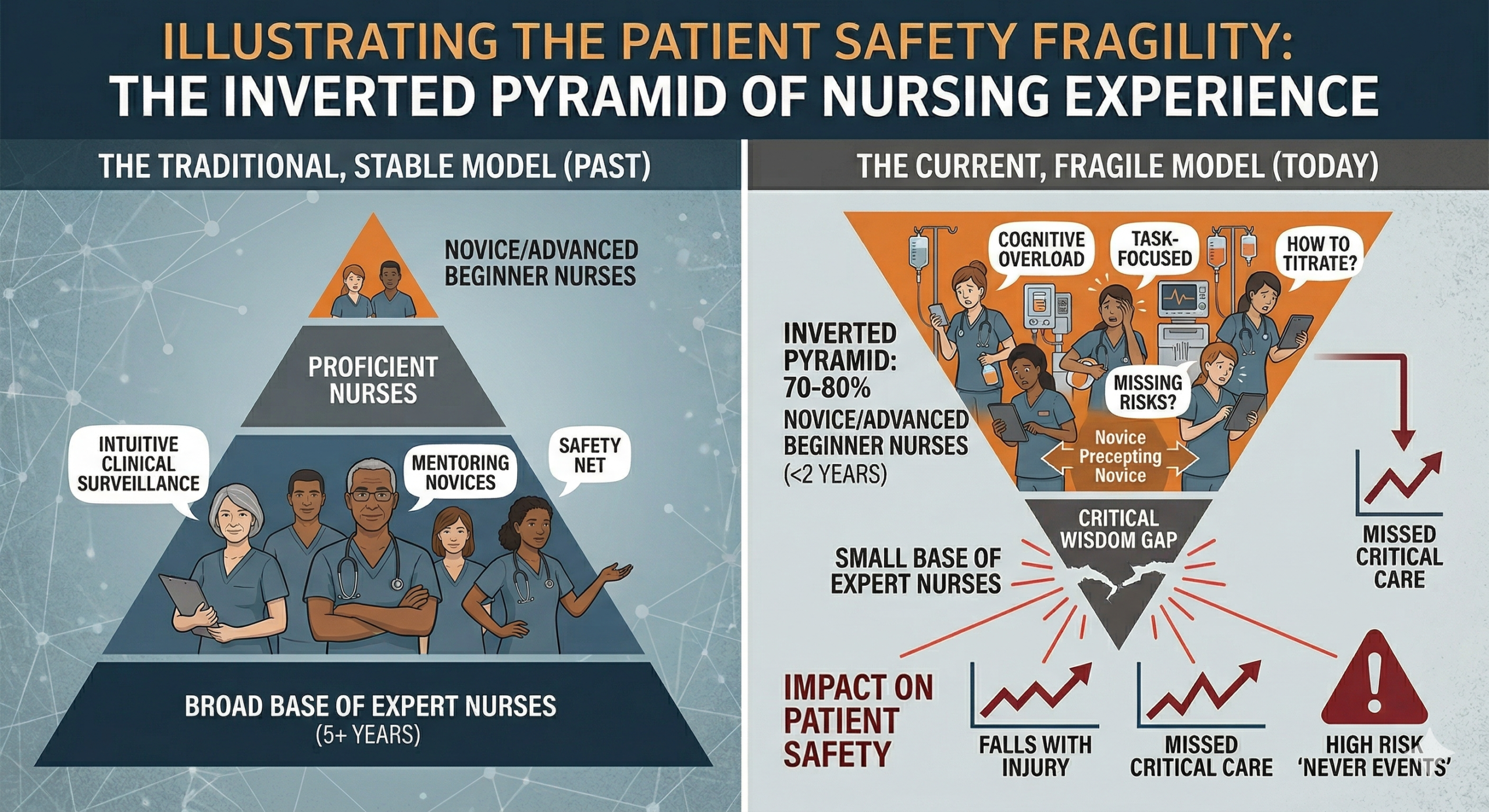
For decades, the “pyramid” of nursing was stable. We had a broad base of expert and proficient nurses who mentored a smaller group of novices. Today, that pyramid has been flipped on its head. In many units, 70% to 80% of the staff are now “novice” or “advanced beginner” nurses with less than two years of experience. These are dangerously high numbers from a quality-risk perspective. When most of your frontline staff are still learning to “read the room” clinically, the safety net that used to exist—that intuitive “sixth sense” of an experienced nurse—is stretched incredibly thin.
How Nurse Experience Impacts Safety
-
The Loss of Clinical Surveillance: Expert nurses don’t just follow checklists; they recognize subtle patterns of deterioration before a “Code Blue” is ever called. In an Inverted Pyramid, we have fewer eyes capable of that high-level surveillance.
-
Cognitive Overload: Novice nurses spend a great deal of their time and mental energy on tasks (how to titrate this drip, how to document this assessment). When your brain is maxed out on the “how,” it’s much harder to focus on the “why,” leading to errors in clinical judgment.
- Novice Nurses Leading Novice Nurse: We now see novice nurses taking charge in their first year of practice. It is not unusual for preceptors to have only six months of experience when they guide other novice nurses. There is very little transfer of safety wisdom happening because the wisdom is not there to share.
System Issues Impacting Patient Safety
- Throughput as a Safety Tax: While we have more nurses, the velocity of patient turnover is so high that the “admission-to-discharge” cycle never allows a novice nurse to establish a clinical baseline for their patient.
- The “Checklist” Fallacy: C-Suites love dashboards. But the reality is that novices think differently and focus on “tasks.” This is difficult to quantify and sometimes even to explain to others in the C-Suite. We are seeing high compliance with documentation (the checklist) but a decline in surveillance (the patient). The metrics remain flat because we can’t quantify the impact of a decline in surveillance on patient safety in a novice workforce.
- The Tech Debt: Often, the very technology meant to save us is actually a “cognitive tax” on the novice who is already overwhelmed by the “how” of basic care.
Patient safety is harder today because the clinical wisdom gap is wider than ever. We are asking a generation of young nurses to carry a level of complexity that would have challenged experts twenty years ago. It is not surprising that they are not assessing risk in the same way, and judgment errors are increasing. It is also not surprising that missed care is on the rise, and that some missed care is critical to patient outcomes. Falls with injury are skyrocketing across the country, as novice nurses are less attuned to the risks that patients may present. The safety nets that once existed with larger numbers of experienced staff no longer exist in many units.
When a vacancy is filled with a novice today, we are looking at a 12-to-18-month lead time before that nurse provides a “Safety ROI.” We are currently in a “Knowledge Deficit” that cannot be solved by hiring alone; it requires intentional, structured models for the transfer of wisdom. We cannot continue to treat nurse residency as a ‘finish line’ for orientation. In an Inverted Pyramid, residency must be the beginning of a multi-year ‘Wisdom Residency’ where the few remaining experts are protected and deployed specifically as clinical ‘Air Traffic Controllers’—not as bedside providers, but as the safety net for the novices who now hold the line.
Are your leaders leading in an Inverted Pyramid and struggling to meet their patient safety metrics? Consider booking our workshop on this topic. This workshop has a strong ROI and is appropriate for all levels of nurse leaders, including charge nurses and NPD professionals.
The Inverted Pyramid: Leading Teams of Novice Nurses The Inverted Pyramid WS Information Sheet
© emergingrnleader.com 2026
To effectively lead through these challenges and others, nurse leaders need new tools and strategies. Let me help you as I have helped hundreds of organizations over the past five years. Book a workshop or keynote for your team by contacting me at roseosherman@outlook.com
Brand New For 2026 and Already Receiving Rave Reviews – Staying Power Building a Culture of Retention in the New World of Work
Our Most Popular Right Now –The New World of Work Workshop
A Leader Favorite – Building Bridges Not Walls: Leading Multigenerational Work Teams – Click Here for More Information Building Bridges Not Walls
A Must-Read Book in 2026 – Click Here to Buy



 LinkedIn
LinkedIn