By Rose O. Sherman, EdD, RN, NEA-BC, FAAN
I have been thinking a lot recently about the drivers for both nurse leader and workforce burnout and exhaustion. What has changed in this post-COVID environment that has brought us to where we are today? Will money and more staff solve the problem as unions suggest?
There is so much complexity in what we see in healthcare today that the answers are nuanced. Some challenges can be addressed through a focus on healthier work environments or more staffing, but not all. Younger staff view their careers differently and have made it clear that they will not have careers bound to any one unit or department. Nursing leaders will need to design new care-delivery structures to respond to the Inverted Pyramid we now see on so many nursing units, while also reconsidering their own leadership.
Viewing Current Challenges Through a Situational Leadership Lens
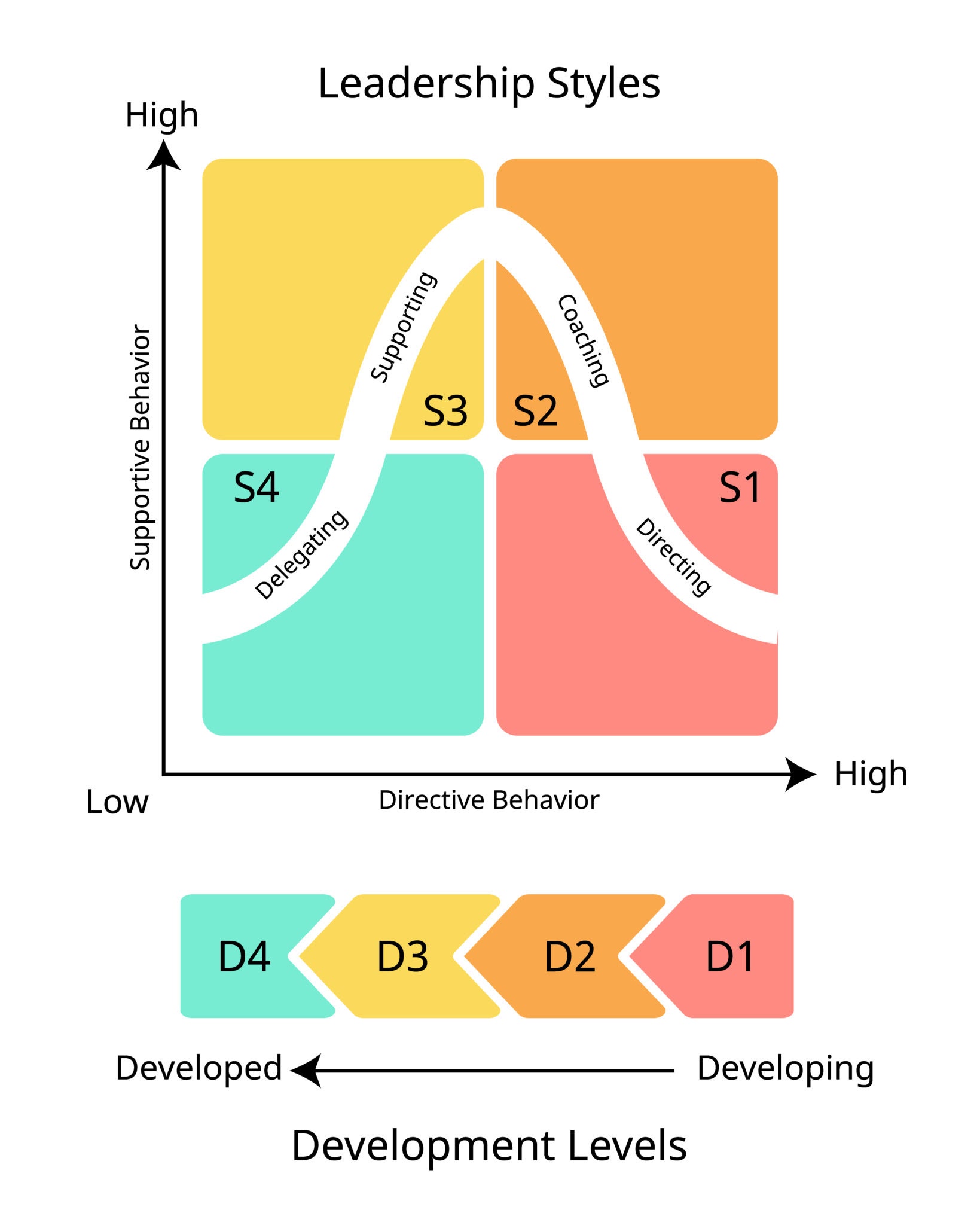
Up until two decades ago, situational leadership, as originally conceptualized by Hershey and Blanchard in the late 1960s, was widely taught in nursing leadership programs. The underlying principle of the framework is that effective leaders adjust their leadership behavior based on the developmental level of their staff in three key areas: the complexity of the tasks being assigned, the staff member’s competence to do what is being asked of them, and the staff member’s confidence level. In situations where complexity is high but competence and confidence are low, leaders need to be more hands-on and provide closer supervision. When staff are more experienced and confident, you can delegate more and move to an empowering approach.
Situational leadership was, at that time, viewed as a framework for analyzing the leader’s work and could be accompanied by a preferred leadership style, such as transformational, human-centered, or transactional. As graduate students in nursing leadership, we were taught that leadership is complex and much of what you may need to do is driven by the context of the leadership situation you are in. Situational leadership provided an approach to thinking about leadership work through the lens of workforce needs.
What Happens with an Inverted Pyramid?
Recently, I have been thinking about how Situational Leadership and the Inverted Pyramid intersect. For decades, nurse leaders were fortunate to have a workforce that Hershey and Blanchard would have characterized as highly ready to accomplish what was being asked of them. Nurse leaders only needed to direct and coach a small number of nurses. Broader spans of control were possible in that environment.
Fast forward to today, and the majority of nurses on many acute units have much lower levels of readiness and require more hands-on leadership on the right-hand side of the situational leadership quadrant. These large spans of control that once worked are leaving our frontline nurse managers exhausted and burned out. We once had a workforce structure where being a servant leader was enough – today, that is no longer true. When you have an experienced workforce, your primary job is servant leadership. You aren’t there to tell people what to do; you are there to remove the barriers that prevent your team from providing excellent care. You can expect a high level of involvement in professional governance.
What is Different Today?
With the Inverted Pyramid, nurses now join teams where they are surrounded by novices like themselves. They are entering healthcare environments with soaring patient volumes, rapid turnover, and high acuity. They lack both critical thinking and technical skills. It is unsurprising that nurse leaders find themselves doing more and more coaching and directing as the number of experienced nurses in practice declines.
Skilled coaching has become a critical competency today due to workforce readiness issues. As they round today, nurse leaders regularly ask themselves: Does this nurse need me to show them how (Coaching), or do they just need me to get them the supplies they’re missing (Supporting)? The answer often is that the nurse needs to be shown how to do something – and that takes time. Nurse leaders spend more and more of their time in the right quadrant of the situational leadership model.
Situational Leadership and the Nurse Manager Role
We often talk about nurse manager roles as if they are all the same, but nothing could be further from the truth. If you look at high-turnover areas today, such as Medical-Surgical Units, ICUs, Telemetry, and Emergency Departments, these managers have to lead differently than managers with significant numbers of experienced staff. Their staffing pyramid is inverted, and that is unlikely to change in the near future. They have no choice but to look at their leadership situationally. They find that the staff needs more from them because they lack the skills and readiness needed to perform their roles independently.
As we look to restructure nursing, whether it be spans of control or where to introduce virtual nursing, we should consider whether the unit has an Inverted Pyramid and where leaders spend time in the Situational Leadership Quadrants. All unit teams are not alike, and neither are their leadership needs.
© emergingrnleader.com 2026
To effectively lead through these challenges and others, nurse leaders need new tools and strategies. Let me help you as I have helped hundreds of organizations over the past five years. Book a workshop or keynote for your team by contacting me at roseosherman@outlook.com
Brand New For 2026 and Already Receiving Rave Reviews – Staying Power Building a Culture of Retention in the New World of Work
Brand New for 2026 and Already Popular – The Inverted Pyramid: Leading Teams of Novice Nurses The Inverted Pyramid WS Information Sheet
Our Most Popular Right Now – The New World of Work Workshop
A Leader Favorite – Building Bridges Not Walls: Leading Multigenerational Work Teams – Click Here for More Information Building Bridges Not Walls
A Must-Read Book in 2026 – Click Here to Buy



 LinkedIn
LinkedIn