By Rose O. Sherman, EdD, RN, NEA-BC, FAAN
As I look at the landscape of acute care today, I see a profound shift that keeps many leaders up at night. We are leading a workforce with a high concentration of novice nurses—talented, eager, but fundamentally lacking the “clinical mileage” that seasoned veterans rely on. When we talk about patient safety in this context, we often default to broad terms like “culture” or “staffing ratios.” But a recent study in Research in Nursing & Health provides us with the specific clinical “missing link” we’ve been looking for: Nursing Surveillance. It turns out that a favorable work environment doesn’t just make nurses “happier”—it directly enables the frequency and quality of nursing surveillance, which is the engine that drives patient safety.
Nursing surveillance is more than just checking a box; it is the “continuous, purposeful acquisition, interpretation, and synthesis of patient data to detect early deterioration”. It is the difference between seeing a heart rate of 110 and recognizing it as the first sign of an impending crisis. The challenge for our novice nurses is that surveillance frequency is significantly tied to years of experience. Veterans have a built-in “anticipatory reasoning” that tells them when to walk into a room. Novices don’t have that yet. They need “scaffolding”—structured tools and, more importantly, a leadership structure that protects their time and attention while they build that clinical intuition. Adding staff to units may not improve nursing care if vigilance is not the primary priority.
If the frontline is “thin” due to a lack of experience, the leader must be “heavy” on support. The study used the PES-5 scale to measure the work environment, and the results are a roadmap for any nurse manager looking to more effectively hardwire vigilance into care.
- Protect “Sustained Attention”: Surveillance is demand-sensitive. When a unit is understaffed or chaotic, the cognitive load erodes a nurse’s attentional resources. Novices today already struggle with focus and prioritization. Leaders must protect young nurses from non-essential interruptions. If a novice is distracted, they miss the subtle cues of deterioration.
- Provide Responsive Leadership: The research found that an “administration that listens and responds to nurse concerns” is a primary pillar of a safe environment. For a novice, this is about psychological safety. They need to know that if they escalate a “gut feeling” based on their surveillance, they will be met with support, not skepticism.
- Strengthening Professional Relationships: Good working relationships between doctors and nurses are essential for the “escalation of care”. As leaders, we must facilitate these relationships so that when a novice detects a change, the pathway to action is clear and respectful. So many leaders tell me that their physicians have taken to complaining about the nursing staff’s lack of competency. If this is the message sent when a novice escalates a concern, it will undermine unit surveillance and the nurse’s confidence.
Actionable Tools for Novice Nurses
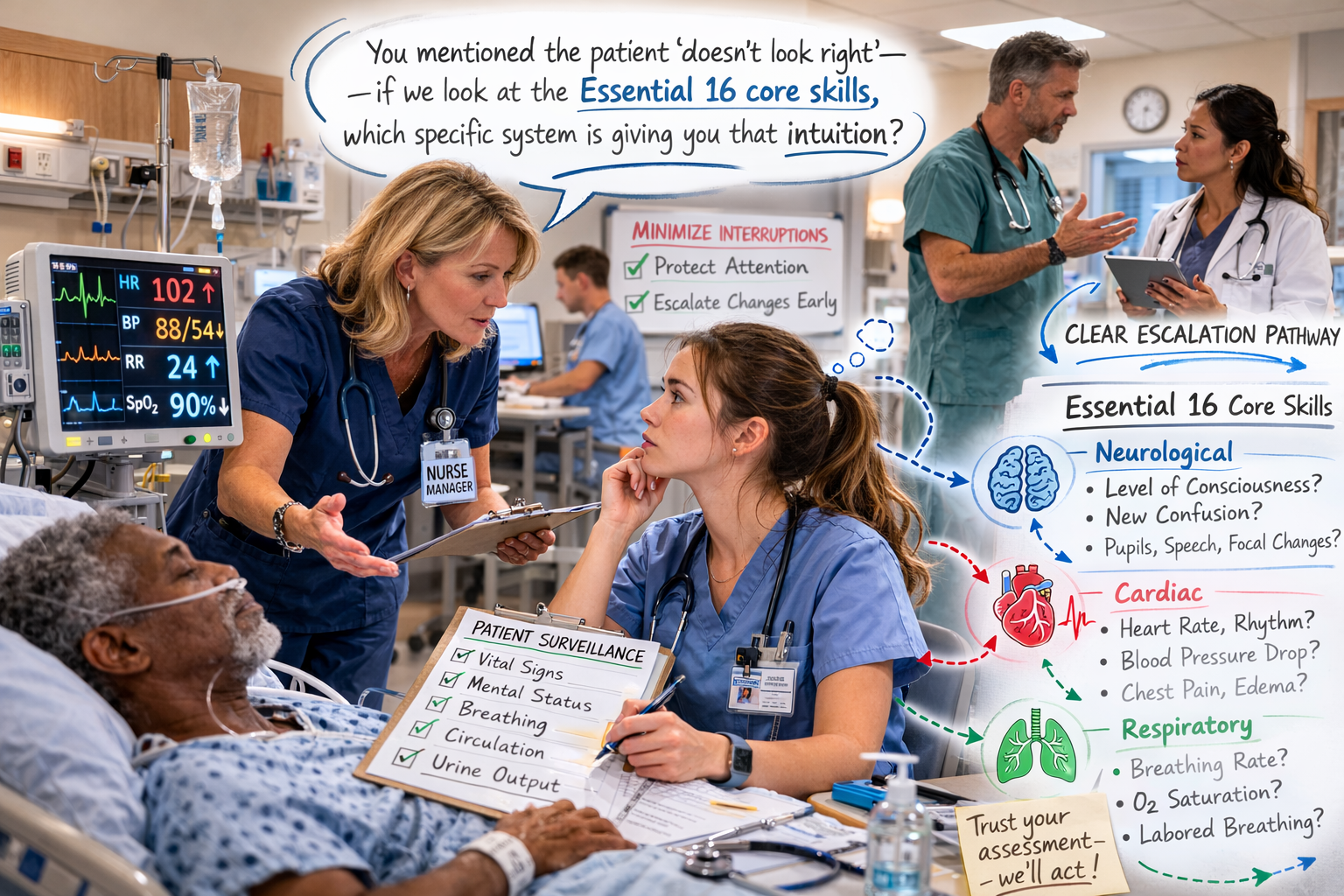
We cannot simply wait for novice nurses to gain ten years of experience. We have to give them the tools to provide surveillance at a higher level today. One way to do this is by focusing on the 16 core physical assessment skills for medical-surgical safety that novices should be continuously monitoring:
Respiratory: Airway patency, rate, effort, saturation.
Circulation: Pulse rate/rhythm, BP (by auscultation if needed), and urine output.
Neurological: Level of consciousness and speech evaluation.
Physical Integrity: Pain assessment, skin integrity/pressure injury inspection, and wound/drain observation.
Mobility/Elimination: Ability to transfer/mobilize and have bowel movements.
By standardizing these 16 skills—from measuring respiratory rate to assessing speech clarity—we provide the “data acquisition” framework that novices need. But we must go further. We need to teach them synthesis. We should encourage them to ask: Is this different from four hours ago? Do these three subtle changes suggest a trend?.
-
Does my staffing truly allow for the “Essential 16” assessments to happen every shift? Do my novices know that these are the essential 16 assessments they should continually monitor for change?
-
Do I look for ways to reduce distractions in my unit, such as hunting for supplies and equipment rather than focusing on patient assessments? Have I implemented “No-Interruption Zones” or policies to protect the sustained attention required for systematic clinical surveillance? Do I consider factors such as student assignments for novice nurses with weaker clinical surveillance skills?
-
When I make leader rounds, am I using my conversations with my novice staff to strengthen their surveillance skills?
-
Have I created a culture where a novice feels “free to question decisions of those in authority”? How do I manage conversations with irritated physicians about calls they may receive from novices in a learning mode?
-
Do I create psychological safety about errors in surveillance? If a nurse detects a change but misses the “window” for early intervention, do we discuss it as a system-level learning opportunity rather than a personal mistake?
-
Are we investing in and evaluating every new technology that streamlines data to help nurses see patterns rather than just numbers?
As nurse leaders, we need to be explicit with new staff today that nursing surveillance is a key role that nurses play in an acute care environment. Many novices see their work as a series of tasks and miss this critical aspect of their role. Efforts to improve patient safety require a dual approach: structural enhancements to the work environment and targeted strategies to strengthen proactive nursing surveillance.
Reference
Connell KA, Yu H, Villani D, McHugh MD, Douglas C. The role of surveillance in the association between the nurse work environment and patient safety culture. Res Nurs Health. 2026;49(1):1-11. doi:10.1002/nur.70056
© emergingrnleader.com 2026
To effectively lead through these challenges and others, nurse leaders need new tools and strategies. Let me help you as I have helped hundreds of organizations over the past five years. Book a workshop or keynote for your team by contacting me at roseosherman@outlook.com
Brand New For 2026 and Already Receiving Rave Reviews – Staying Power Building a Culture of Retention in the New World of Work
Brand New for 2026 and Already Popular – The Inverted Pyramid: Leading Teams of Novice Nurses The Inverted Pyramid WS Information Sheet
Our Most Popular Right Now –The New World of Work Workshop
A Leader Favorite – Building Bridges Not Walls: Leading Multigenerational Work Teams – Click Here for More Information Building Bridges Not Walls
A Must-Read Book in 2026 – Click Here to Buy



 LinkedIn
LinkedIn